


What is Patellofemoral Pain Syndrome?
PFPS is an umbrella term for pain in and around the patella (kneecap). It is sometimes called “runner’s knee” or “jumper’s knee” because it is common in people who run or play sports, but it can affect anyone.

PFPS is most commonly caused by vigorous overuse of the knee, and jogging, squatting, even climbing stairs can be culprits. Suddenly changing or increasing the amount of physical activity you do can also put excess stress on the knee, leading to PFPS, as can using inappropriate equipment or footwear. PFPS can also be caused by incorrect alignment of the patella.
If you’re experiencing PFPS, you’re likely to have pain in your knee that gets worse when you sit, climb stairs, run or squat. The pain can be felt anywhere around the knee.
What can you do about PFPS?
If you’re experiencing pain in your knee that you think could be PFPS, stop doing the activities that are causing you pain until you feel better. This might mean switching to low impact exercise for a while. Use the POLICE method:
Protect – avoid making the painful knee worse by stopping the activity you are doing
Optimal Loading – keep moving the joint as pain allows (don’t become a couch potato!)
Ice – use cold packs for 20 minutes, two to three times per day
Compression – a knee bandage can help prevent swelling (your physio can advise on the best one)
Elevate – whenever you can, rest with your knee supported in a position higher than your heart
See your physiotherapist to check the severity and type of the injury and see what needs to be done to help you recover.
How can a physiotherapist help with Patellofemoral Pain Syndrome?
Your physio will examine you to determine exactly what is causing the pain and where the specific problem lies. As there are a number of tendons and muscles in this area that could be affected, you need to know exactly what the problem is before it can be addressed.
Depending on the nature of your problem, there are a range of exercises that your physio might suggest to help strengthen and stabilise the area, as well as helping you regain movement. Manual therapy and massage may also help reduce pain and recover motion.
Your physio will be able to advise as to whether you need any bandages, taping or support equipment, and which ones are right for you. They will also advise on whether you’re wearing the right shoes, using the right equipment and following the best training regime to reduce the likelihood of the problem coming back.
Frequently, the muscle synergy around the knee becomes altered. The cortical representation of the muscle attaching to the inside of the knee cap (vastus medialis) is frequently diminished and relocated to another aspect of the cortex, making normal muscle contractions very difficult. Retraining the brain becomes important, to enhance the vastus medialis activity.
see below for further explanation on Cortical Resource Mapping and Game Theory
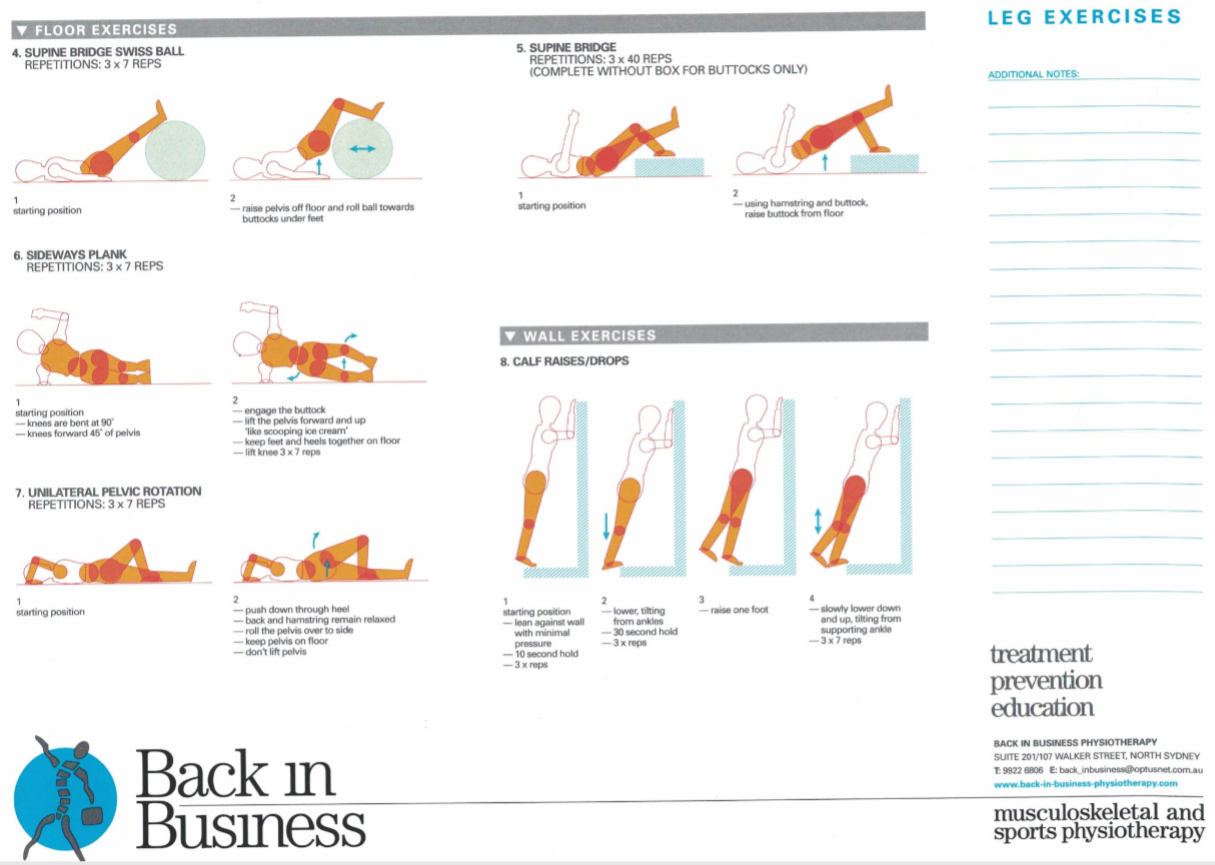
Exercises which are designed to 'unload' the knee joint become important. These include synergistic loading of the upper 2/3 of the hamstrings/quadriceps as well as gluteal activation. Furthermore, calf strength is of paramount importance, as the calf absorb up to 70% of the load when landing on the ball of the foot. Frequently, continuous hopping and skipping are the last functional dynamic exercise outcomes used to determine full return to sporting activity.
- reverse lunges
- sideways lunges
- Swedish squat
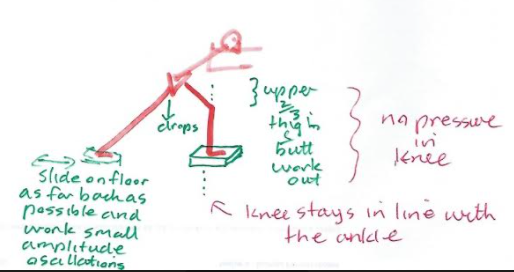
- quads hover
- hip hitches
- core stability and gluteal one legged bridges
- hopping and skipping
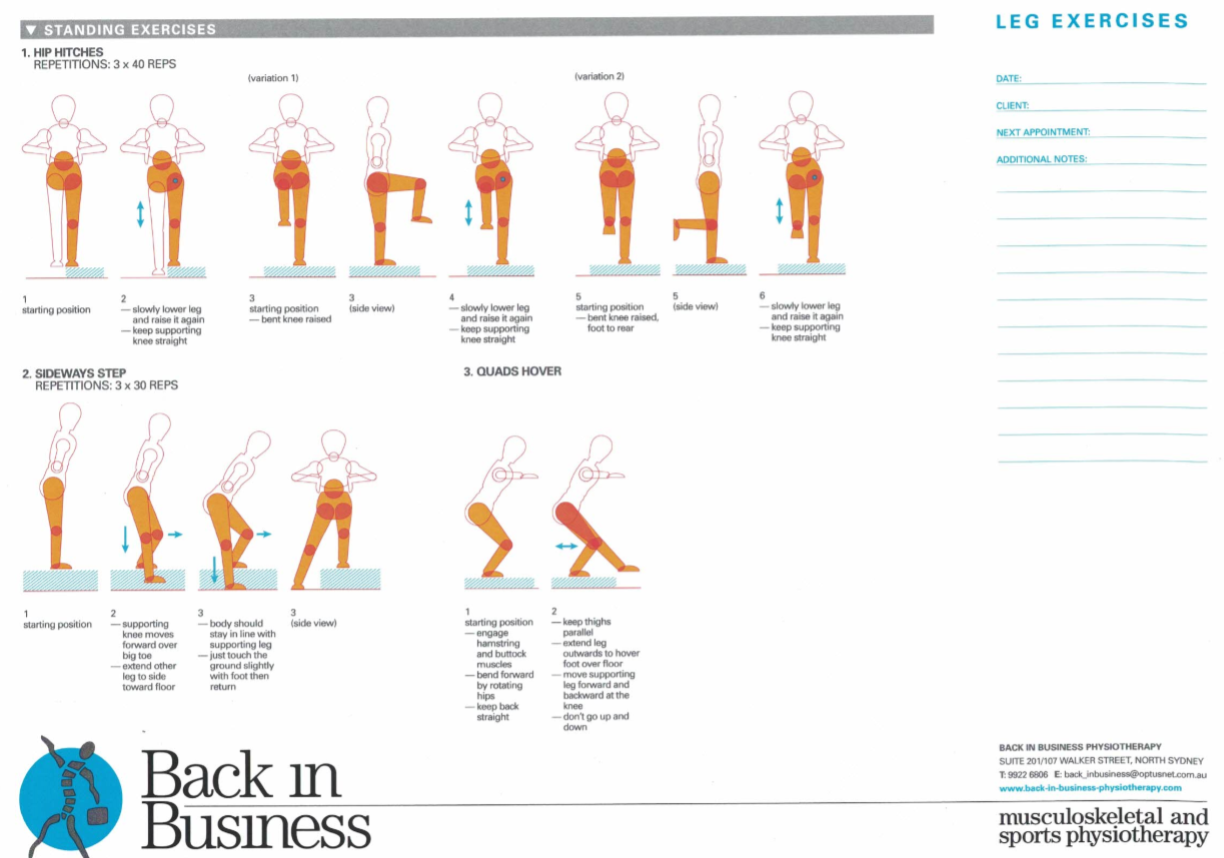
Leaning forward, through the rotation in the hip, with a straight back, should take the pressure out of the knee, whilst doing sideways and reverse lunges, as well as the quads hover. Importantly, with the quads hover, the movement of the knee is forwards and backwards, NOT up and down.
Perfecting reverse lunges, is the precursor to other lunging activity. Progression, should be reverse lunge, diagonal reverse lunge, sideways lunge. Initially using a slider on the floor and ultimately progressing to a small step.
What can you do to prevent PFPS?
If you think you might be at risk from Patellofemoral Pain Syndrome, the best things you can do to reduce your chances of injury are:
- Introduce a new training regime or a change in activity slowly – get physiotherapist advice on putting your activity plan in place
- Get expert guidance to make sure your footwear is appropriate and supportive, and that you’re using any equipment correctly
- Maintain a healthy weight to avoid putting excess strain on your knees
- Warm up thoroughly before exercising
- Stretch your quads and hamstrings before and after exercise
- Don’t push yourself – if you’re exercising and your knee (or anything else for that matter) begins to hurt, stop, and get on the phone to us!
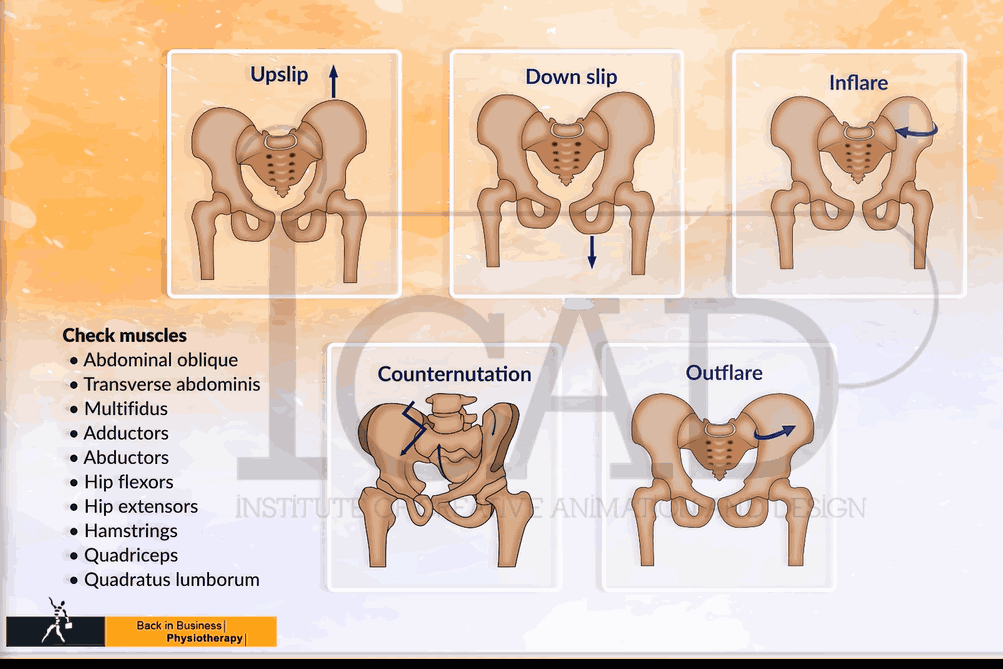
Muscle coordination within and between limbs
Researchers have demonstrated the importance of intra-limb coordination for the development of peak sequential power from knee to hip to ankle, and the reliance on multiple muscles to produce torque. At back in Business Physiotherapy, we use a very comprehensive approach to treating the spine and pelvis, whereby, even improvements in areas of the body not traditionally associated with leg dynamics, such as ribcage biomechanics, will improve power output in the legs. Treatment of pelvic asymmetries and low back conditions can frequently relieve recalcitrant chronic knee pain. These issues have been addressed elsewhere on this website.
Game theory and the curious concept of immune - muscle synergies
It is interesting to speculate that both the novice and elite orienteer are more susceptible to infection because they both have more rigid motor patterns, are less inclined to take risk and therefore are less likely to be confronted with error generating patterns of correctability? The assumption underlying game theory is that there is a resource over which there is a conflict.
A factor which the orienteering paradigm partially defines, and identifies, is the freedom of thought and movement. That fact that many investigations are looking at exercise and the immune system, using captive animals, might be problematic in itself. These animals are in a predictable environment, which for this purpose is ethical, reductionist and conforms with rigorous scientific research protocols, which is practical, as it reduces the number of 'dependent' and 'independent' variables. However, from an evolutionary point of view, and from the perspective of the example used here, where in orienteering, more may be learnt and fine-tuned, in an unpredictable variable environment, whereby the use of caged animals may be limiting the validity of the paradigm (deterministic chaos) which is under investigation. Moreover, in terms of cognition, confinement is a stressor. Moreover, the calmness and clarity of thought needed in the freedom of orienteering (running and navigating) through the landscape can be considered the antithesis of the caged animal.
Our ancestors were striving for energy security through appeasement, subjugation or dominance over other life forms, both internally and externally. In this sense, the 'freedom to navigate and move' paradigm, suggests that our evolutionary forefathers, used their muscles, to propel themselves out of Africa, for 'greener gut biome pastures'. Therefore, maintaining good health in new and potentially 'dangerous environments', involved an unpredictable deterministic variable. As it pertains to cognition, it is an intriguing idea that a motor-sensory curiosity, drove a mechanism, which simultaneously caused muscle hypertrophy, and endowed the muscles with enhanced glutamine and cytokine concentrations, which were needed, if an immune response to pathogens was encountered. Additionally, it is conceivable, that the gut biome was driven by the laws of thermodynamics, in the search for energy. Subsequently, the gut-environment interface provided the interaction needed, to both provide energy for movement, allowed the immune system the encounters needed to flourish, and achieved the abundance of gut species required, in a variety of situations, from feast to famine. Therefore, the gut - muscle - brain cognitive pathway, was driven at a conscious and subconscious level to meet the demands of thermogenesis and immune competency, resulting in collective gain amongst all cells which required energy. Akin to Zen Buddhist philosophy, suggestions are, that the constant sensation of mild hunger, drives the clarity of thought needed, to strive for all encompassing meaning and ultimate enlightenment. Yoga, using animal poses, to stretch muscles and enhance breathing, whilst calming the cognitive state, may be based on the same primeval paradigm, of what is good for muscles is also good for the gut and brain.
The 'dove and hawk' paradigm in game theory is interesting. If a hawk and dove compete over the same resource, direct open conflict of the dove with the hawk would be suicidal. Hence, one would think it's better to be a hawk. However, what if two hawks meet, there will be only one winner and potentially both could be injured for the same net gain. Whereas, if two doves meet, they may postulate and gesticulate and eventually one may retreat or they may even share the resource, with the less risk of injury. Hence, the stakes for the Hawk are much higher. Humans have always been in conflict for resources. Does this mean that the immune system is tuned by adaptation to 'individual' resource dominance? Or, as people developed and evolved as tribes, into communities did our immune systems come to share pathogens, which may have entailed 'herd immunity' but at the same time, gave humans a lack of species variability, making them more vulnerable to 'novel' pathogens? Even more intriguing, is the notion that within a group of similar, the weakest may be driven out, seeking new resources, which in this case means new environments and new pathogens, invoking an 'immune enriching' response?
Continuing with the 'hawk dove' analogy, if we have too many hawks in a population, the consequences are constant conflict. If too many doves, constant compromise. In fact, a single dove in a hawk environment might be totally ignored, as might a single hawk in a dove environment. Thus, the apparent weaker species could be at an advantage when it's the outlier? To carry this further, we could postulate that the hawk is more prone to injury. Does this mean that in humans, the more dominant 'aggressive' individuals have an immune system which is more in demand for potential or actual injury? Whereas, the postulating dove, activates it's immune system minimally when it's performing some form of escape or deception? Interestingly, most animal conflict encounters, go out of their way to avoid injuries to themselves. Regardless, it's likely, that in both 'stressful' situations, the immune and musculoskeletal systems are activated, in a proportionately preparatory manner. Thus, the stronger the variability in the individual, the more proportional, and therefore robust their immune response.
Needless-to-say, a balance between hawks and doves needs to be established for mutual gain to take effect. In terms of the human genome, it's very underwhelming, yet it has evolved to a complex multi-cellular life form, still totally dependent upon trillions of unicellular life forms within the individual gut biome. This flies in the face of Darwinian evolution and the survival of the fittest, in that simple life forms keep complex life forms alive. Even, within the gut biome, there appears to be a symbiotic relationship with parasites and a healthy immune system (i.e. parasitic exposure appears to reduce auto-immune disease such as allergies). A 'simple' multitude (gut biome) balanced with a 'complex' minority (human DNA). Humans eat to feed their gut, their gut breaks down energy from food, which in turns propels the human, with the energy gained, to find more food. A net win win situation using the gut-brain-muscle axis.
In terms of muscles, a simplistic view, (using this analogy) would be that the glycolytic (fast twitch) muscles are the 'hawks', whereas the oxidative (slow twitch) muscles are the 'doves'. The glycolytic muscle fibres tend to be ballistic two joint (mechanical) energy straps which propel the body, whereas the oxidative endurance (metabolic energy) muscles are one joint deep muscles tending to stabilise joints and prevent injury. Therefore, the 'hawks' make the large perturbations whereas the 'doves' dampen them. Luckily, there is a muscle glycolytic fibre type which can become more oxidative (endurance power). Hence, 'hawks' which can be tempered towards a 'dove' like mentality....a balance between metabolic and mechanical energy systems, where the mechanical perturbations stimulate the metabolic-immune response.
In terms of neurophysiology, this analogy could potentially be taken further, where the sympathetic nervous system is the 'hawk' and the para sympathetic nervous system are the 'doves'. Fortunately, within the sympathetic nervous system there are self modulating ('dove' like) perturbating mechanisms. But it could be envisaged that putting a 'hawk' amongst the 'doves' wakes them up from a state of complacency. Similarly, 'staleness' is an 'existential threat' to any training regime and to any 'immune system'. Read more : Muscles, Deterministic Chaos and the Immune System
Cortical 'resource' representation, mapping, in knee muscles, after injury
In the context of physiotherapy, a simple model of game theory might be applied to the problem of anterior knee pain. Commonly, this problem is associated with pain at the front of the knee when it is in flexion (a bent position), such as stair climbing, cycling, squats, etc. The conventional wisdom is that the patella (knee cap) is mal-aligned due to a lack of medial (VMO) muscle activity pulling the patella inwards and too much activity of the lateral thigh muscle (VL) pulling it outwards. Game theory could be applied here as the muscles compete for finite cognitive territory to represent their individual (rather than mutual) function, where ultimately neither muscle gains, both loose out to pain generating cortical representations, reducing fidelity and increasing noise in the system. However, if the muscles were to readjust for a functional outcome, they would do so through gaining a synergy of proportionally shared resources (power sharing), hereby a dominance over pain and dysfunction is gained. Physiotherapists, use functional electrical muscle stimulation (FEMS) to give added 'resources' to the VMO, which then can be used during functional exercise training. As the system adjusts, the pain improves and the gain experienced by all the muscles convinces the VL to fire with the VMO, hamstrings and gluteals in a functional synergy for stairs, cycling (see previous), squats, etc. Hereby, game theory would suggest all have won and injury has been avoided.
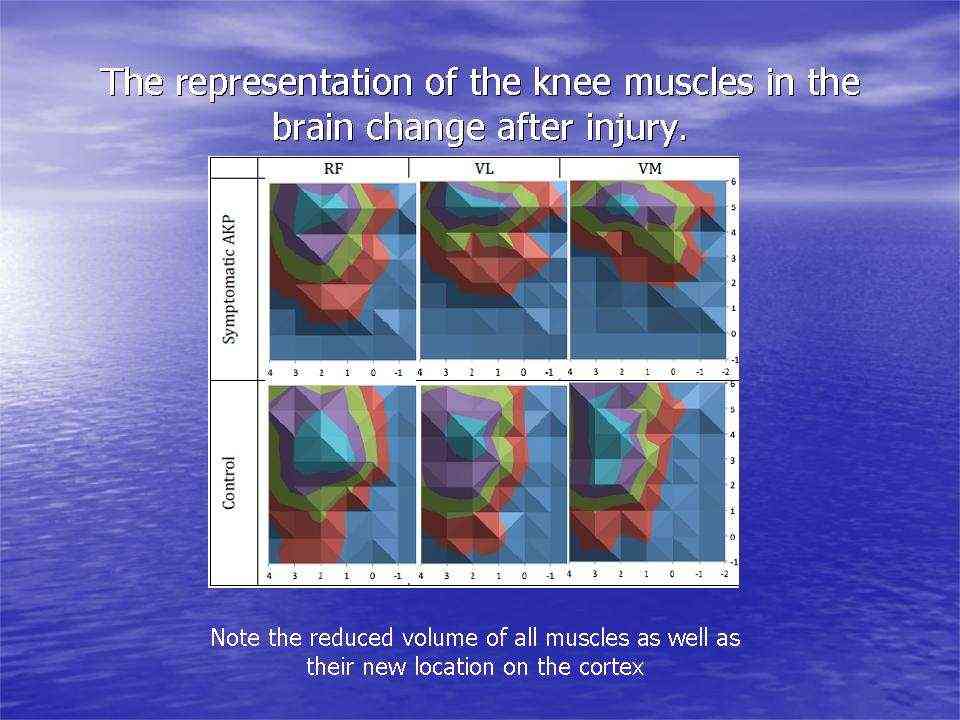
Investigations in Australia, by the Brazilian, Abrahao Baptista (2014), looking at 40-50 year old women with chronic knee pain, demonstrated the significant reduction in the volume of muscle representation in the cerebral cortices, as well as changes in the location of these muscle representations (see below). Moreover, in the context of neurons who 'fire together, wire together' it would be of utmost importance to find exercises that act as functional synergies and relate in a real or a 'virtual' manner to the environmental context in which they need to fire. This also becomes particularly important in psychological behavioural issues of 'fear avoidance' and disuse atrophy. Ideally rehabilitation stimulates 'wiring and firing together' of goal-oriented regions of the brain rather than those which are directed at fearing and avoiding movement. Therapist must instil confidence through their choices of treatment whereby they outline and hence monitor the expectations of outcome.
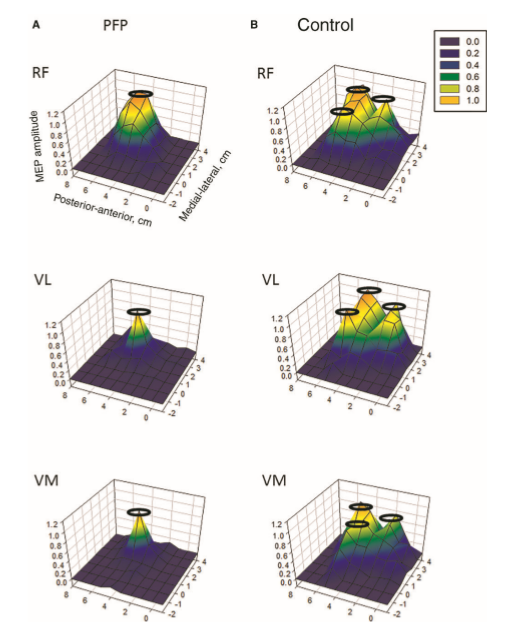
In this picture, it is clear that, the volume of the quadriceps muscle representation in the cortex of people with anterior knee pain (PFP = patello femoral pain) is dramatically reduced. Not seen here, but demonstrated in other research, is the phenomenon of pain processing altering cortical activity in various brain areas (see below).
Individuals with patellofemoral pain (PFP) had reduced map volumes and an anterior shift in the M1 representations, greater overlap of the M1 representation and a reduction in cortical peaks across all three quadriceps (RF, VL, VMO) muscles compared with controls.(Te et al 2017 Pain Medicine, pnx036, https://doi.org/10.1093/pm/pnx036). Physiotherapists use FEMS (30HZ functional electromuscular stimulation) to enhance muscle cortical representation in the brain, which improves function and in turn improves pain. FEMS stimulation readjusted cortical mapping to that seen in asymptomatic individuals. Alternatively, therapists use trans-cortical stimulation of the pre-frontal cortex to improve 'executive function' and pain.

Brain activation related to spatial discrimination of noxious stimuli is distinct from that related to perceived pain. These images are located at x = 0 mm, x = 30 mm, z = 5 mm, and y = –30 mm in standard stereotaxic space. IPL/SPL, Inferior parietal lobule/superior parietal lobule; GP/PT, globus pallidus/putamen; M1, primary motor cortex; DISCRIM., discrimination. (Oshiro et al 2007 J Neuroscience, 27, 13, 3388-3394)
Abrahao Baptista (2020) and his colleagues are conducting research into trans-cortical stimulation and vagal (para-sympathetic) nerve stimulation in the treatment of patients with COVID-19. They are basing their assumptions and working hypothesis on some positive results a rheumatologist has had with this methodology for the treatment of auto-immune inflammatory disease. COVID-19 has many of the hallmarks of an auto-immune disease, including the cytokine storm. This treatise has argued that sympathetic, rather than para-sympathetic, stimulation is necessary to add a deterministic chaotic input which perturbs the immune system into action. It would be intriguing to speculate a large perturbation between sympathetic and para-sympathetic can also activate the immune response. In this case, the illness has already set the sympathetic nervous into a heightened chaotic state, which needs additional buffering (redundancy) from the vagal nerve stimulation.
References
1. Physiopedia. 2021. Patellofemoral Pain Syndrome [Onlinehttps://www.physio-pedia.com/Patellofemoral_Pain_Syndrome
2. OrthoInfo. 2020. Patellofemoral Pain Syndrome [Onlinehttps://orthoinfo.aaos.org/en/diseases--conditions/patellofemoral-pain-syndrome/
Uploaded : 23 January 2022
Updated : 7 April 2022
